If it was your child, what would you do?
This is a question that drives many of our doctors and nurses to give your child the best possible care while you are here. If your child is at our hospital, you trust us to help get your child well so you can go home. Sometimes there are risks associated with those treatments, though. We strive to avoid unnecessary risks and minimize necessary risks.
One such example: 70-80% of all inpatients require IV access (or intravenous access) to administer either fluids or antibiotics at some point during an inpatient stay. Since these peripheral IV’s have to go into a vein, there is a slight possibility of the tube coming out of the vein and the fluid going under the skin instead. This complication is called extravasation. If there is an extravasation with certain medications and it is not attended to immediately, it can cause very serious harm to the patient, resulting in possible surgery and, in some cases, even skin grafts.
To prevent these complications, Dr. Neil Johnson, one of our interventional radiologists and the Vascular Access Chief, led a team to develop a standard for Cincinnati Children’s to follow. This team, called iVAG (Infusion and Vascular Access Governance), consists of 15 senior doctors and nurses from various specialties around the hospital. It took years of research and documentation, and we now have a system set in place to protect our patients.

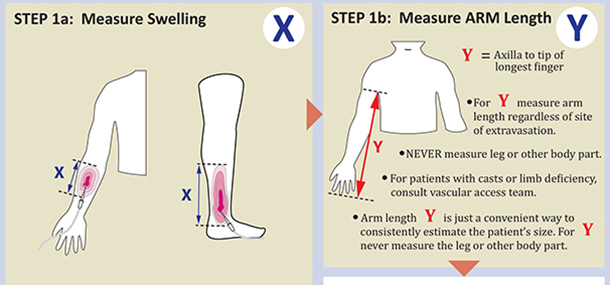
When an IV is being used, nurses on the floor have to check the insertion site every hour. They check for swelling by comparing the IV site to the other extremity. If there are signs of swelling, the nurse will measure the area of swelling and then measure from the armpit to the fingertip.


These measurements are entered into the computer system. If the measurements calculate to a number higher than 30%, the Vascular Access Team along with Dr. Johnson and several other senior people are paged immediately. Depending on the medication being used, different steps will be taken to ensure the patient does not suffer serious harm.
For example, medications for cancer are very strong and will do faster damage to the skin and surrounding tissue than that of normal saline, so each will prompt a different response. To ensure an appropriate response, a card was created and posted at every computer that ranks medications into three categories of potential harm to the surrounding tissue. These cards are updated every year to include new medications. Green is mild, like saline, while yellow is moderate and red is severe harm medications, and this is where cancer medications and the like are ranked.
Our system works so well, 88 hospitals across the United States and Canada have adopted it to use in their facilities. Where other children’s hospitals average 6-8 serious harm extravasation events per year, we have only had 1 in the last 5 years and it involved a “red” medication. This incident was thoroughly investigated and we are confident that it will not be repeated.
We take your child’s care and well-being very seriously. Many of our radiologists go above and beyond by collaborating with other areas of the hospital to improve patient safety and develop new standards of care to make sure we are always consistent and doing our very best for you and your child.
Contributed by Dr. Neil Johnson and edited by Sarah Kaupp (RRA).
Alex is a radiologist and the Neil D. Johnson Chair of Radiology Informatics. In this role, he helps to manage the information systems used by the Radiology department. Clinically, Alex is the Assistant Director of thoracoabdominal imaging. His research interests include liver disease, liver tumors, inflammatory bowel disease, and appendicitis.